소아청소년(0~18세) 우울증, Children and adolescents (0-18 years old) Depression
소아청소년 우울증의 개요와 통계
여기서 “소아들”는 태어나서부터 사춘기가 오기 전 아이들을 의미한다.
태어나서부터 사춘기가 오기 전까지 기간을 소아기라고 한다.
즉 사춘기 이전 아이들을 편의상 소아들이라고 한다.
소아청소년은 0~18세 아이들을 의미한다.
우울증은 남녀노소 빈부귀천을 가르지 앓고 사회각계 각층 누구에게나 생길 수 있는 위중한 정신 질환 중 하나이다.
- 소아기에 심한 우울증을 한번이라도 앓으면 그 후 5년 이내 우울증이 재발될 수 있다. 사춘기 이전 소아들이나 사춘기 아이들에게 양극성 정신장애(Bipolar disorder)가 1994년 이래 40베나 증가했다 (출처- Dr. Mark Olson, The Journal of archives of general psychiatry 2007).
- 소아청소년(0-18세)들 10명 중 1명이 우울증에 걸릴 수 있다.
- 사춘기 아이들의 4~18%이 우울증에 걸린다고 한다.
- 심각한 정신병을 갖고 있는 미 사춘기 아이들 중 30%가 치료를 받고 있다.
- 심각한 정신병을 가진 성인들의 50%는 14세부터 시작된다고 한다.
(출처; Journal watch pediatrics and adolescent medicine, August 2008. p769)
- 우울증의 주증은 느낌과 행동 장애가 생기고 건강 상태가 전반적으로 이상해질 수 있다.
- 우울증에 걸린 대부분의 사춘기 아이들은 적절히 곧 치료받지만 우울증에 걸린 일부의 사춘기 아이들은 자기가 우울증에 걸려 있는 줄도 모르고 때로는 부모들도 자녀가 우울증에 걸려 있는지 잘 모르고 있다. 때문에 우울증에 걸려 있는 사춘기 아이들 중 일부는 우울증 치료를 받지 않는 다.
- 또 우울증 치료를 받으라고 권장해도 치료를 받지 않는 경우도 있다.
- 사춘기 아이들의 우울증은 자살의 주원인이 된다.
- 자살은 15~24세 연령층 사춘기 아이들과 젊은 성인들의 사망의 3번째 원인이다.
- 15세 사춘기 아이들의 3번째 사망의 원인이 자살이다.
- 우울증이 있는 사춘기 아이들의 ⅔는 여러 가지 이유로 정신과 전문의 치료를 받지 않고 있는 실정이다.
- 음주, 알코올 중독, 습관성 약물 남용 등은 우울증으로 인해 생길 수 있다. 그와 반대로 알코올 중독이나 약물 남용으로 우울증이 생길 수 있다.
- 사춘기 아이들의 우울증을 적절히 치료받지 않으면 알게 모르게 증상 징후가 점점 심해지고 일상생활 속에 깊이 스며들고 결국 일상생활을 정상 적으로 수행하지 못하고 전 생애가 망치게 될 수도 있다.
소아청소년 우울증 증상 징후 진단
- 다음에 설명하는 1~11항 증상 징후 중 적어도 5가지나 5가지 이상의 증상징후가 있거나
- 그 증상 징후가 적어도 2주 이상 계속되거나
- 그 증상 징후의 정도가 심하거나
- 그 증상 징후로 일상생활을 정상적으로 수행할 수 없으면 우울증이 있다고 진단할 수 있다.
1.
- 죽음에 대한 생각을 하거나
- 죽고 싶은 생각을 하거나
- 죽어가고 있다고 생각하기도 하고,
- 자살로 죽는 방법을 생각하거나
- 때로는 자살을 기도 한다.
- 이렇게 죽는 것을 생각하는 우울증의 증상징후가 나타나면 의사와 즉시 상담진료를 받든지 병원 응급실로 데리고 가서 정신과 치료를 받아야 한다.
2.
- 슬프게 생각하거나
- 희망이 없다고 생각하거나
- 이유 없이 우는 증상 징후가 계속될 수 있다.
3.
- 자존심이 결여되고
- 아무런 이유도 없이 죄책감에 사로잡히고
- 나는 더 이상 좋은 인간이 아니라고 느낀다.
4.
- 살아간다는 것은 아무런 의미도 없고
- 나에게는 앞으로 더 좋은 것이 생기지 않을 것이라고 생각한다.
5.
- 아무 느낌이 없다.
6.
- 전에 아주 좋아했던 공부나 사회활동, 육체활동, 과외활동 등에 흥미를 잃고
- 친하던 친구들과 더 이상 어울리지도 않고
- 혼자서 외롭게 시간을 보낸다.
7.
- 무엇을 할 때 결정하는데 어렵고
- 아예 새로운 일은 시작하지 않거나 할 수 없고
- 기억력이 확실히 상실되고 정신집중을 잘 할 수 없다.
8.
- 신경이 예민해지고
- 사소한 일에 화내고
- 과잉 반응을 한다.
9.
- 보통 이상으로 잠을 과도히 많이 자거나 적게 잘 수 있고
- 보통 이상으로 음식물을 많이 먹거나 적게 먹을 수 있다.
- 체중이 비정상적으로 증가되거나 감소된다.
10.
- 특별한 이유가 없이 항상 피로하다.
11.
- 우울증에 걸린 사춘기 아이들 일부에게 약물남용, 알코올 중독, 무분별한 이성관계, 학교 문제, 성적 불량 등 문제가 있을 수 있고,
- 가족이나 친구와의 관계에 문제가 생길 수 있고
- 권위자나 부모에게 반항적이고 파괴적일 수 있다.
소아청소년이 우울증에 걸렸다고 의심되면
① 가족들이나 친구들 중 믿을만한 사람에게 우울증에 걸린 것 같다는 사실을 말하고 우울증 치료를 받을 수 있는 전문가나 의사와 상담한다.
② 그렇지 않으면 소아청소년과의 진단 치료를 곧 받는다.
③ 학교 카운슬러, 간호사, 사화복지사의 도움을 받는다.
④ 정신과 전문의의 도움을 받는다.
⑤ 카운슬링을 해 줄 수 있는 자격을 가진 신부, 목사, 또는 랍비의 도움을 받는다.
⑥ 증상 징후가 더 심해지기 전 의사의 도움과 치료를 받는 것이 중요하다.
⑦ 심신이 허약하고 건전한 자존심이 결여되고 학교 공부나 과외활동을 하는데 문제가 생기고 무엇을 잘 해보려고 노력하지 않거나 아예 하지 않는 것이 우울증의 증상징후일 수 있다.
⑧ 우울증이 있는 사춘기 아이들의 대부분은 카운슬링과 상담 치료나 항 우울증 약으로 잘 치료된다.
⑨ 우울증은 비교적 흔한 병이고 남녀노소 누구에게도 생길 수 있다. 우울증에 걸린 것 같으면 곧 전문의의 도움과 치료를 곧 받아야 한다. Blood test may indicate early-onset depression in teens. The Los Angeles Times (4/18/2012), Healy reports
아청소년의 우울증의 치료
우울증 치료에 쓰는 약물
-
- Fluoxetine,
- Sertraline,
- Fluvoxaminine,
- Citalopram,
- Escitalopram,
- Antitriptylin 등 여러 종류가 있다.
- Paroxetine, Imipramine은 치료 효과도 없고 해롭다고 한다. 참조 문헌:http://www.jwatch.org/fw110644/2015/09/18/reanalysis-paroxetine-ineffective-and-harmful-treating?query=pfwTOC#sthash.baZesF4R.dpuf
- 그 중 한 종류나 그 이상 여러 종류의 항 우울증 치료제 중 한 두 가지를 선택해서 치료에 쓸 수 있다.
- 그러나 2008년 2월 Irv Kirsch of university of Hull 연구에 의하면 대부분의 우울증 치료에 쓰는 약물은 심한 우울증 치료에는 효과가 있으나 경증 우울증치료에는 효과가 없다고 한다.
- 중증 우울증(Major Depressive Disorder)은 LEXAPRO(Ecitalopram oxalate)으로 치료하기도 한다.
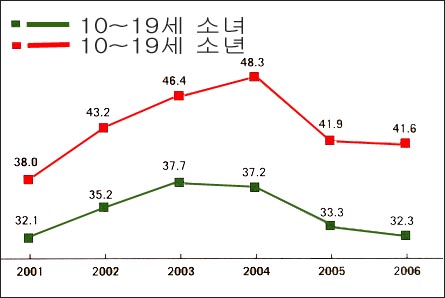
그림 3-249. 우울증 치료제를 쓰는 율은 사춘기 남아들보다 사춘기 여아들에게 더 높다. (위 수는 10~19세 사춘기 아이들 1,000명 중 항우울증 약으로 치료받는 아이들 수) 출처-Medico Health Solutions Inc. and Elsevier Medical News, 2007
Children and adolescents (0-18 years old) Depression
Overview and Statistics of Depression in Children and Adolescents
Here, “children” means children from birth to before puberty.
The period from birth to puberty is called childhood. In other words, children before puberty are called children for convenience. Children and adolescents refer to children aged 0 to 18 years old.
Depression is one of the most serious mental disorders that can occur to anyone from all walks of life, regardless of age or gender.
• Depression can recur within 5 years after having suffered from severe depression at least once in childhood. Bipolar disorder in pre-pubertal and adolescent children has increased by 40 VND since 1994 (Source—Dr. Mark Olson, The Journal of archives of general psychiatry 2007).
• 1 in 10 children and adolescents (ages 0-18) may develop depression.
• It is said that 4 to 18% of adolescents suffer from depression.
• Thirty percent of American adolescents with severe mental illness are receiving treatment.
• Fifty percent of adults with severe psychosis begin at age 14. (Source: Journal watch pediatrics and adolescent medicine, August 2008. p769)
• The main symptoms of depression may be feelings and behavior disturbances and general malaise of health.
• Most adolescents with depression get adequate treatment soon, but some adolescents with depression do not even know they are depressed, and sometimes parents do not even know if their child is depressed. As a result, some adolescents with depression do not receive treatment for depression.
• In some cases, even when people are encouraged to seek treatment for depression, they do not receive treatment.
• Depression in adolescents is a leading cause of suicide.
• Suicide is the third leading cause of death among adolescents and young adults aged 15-24 years.
• Suicide is the third leading cause of death among 15-year-old adolescents.
• One-third of adolescents with depression do not seek treatment from a psychiatrist for a variety of reasons.
• Alcoholism, alcoholism, and habitual substance abuse can all be caused by depression. Conversely, alcoholism or drug abuse can lead to depression.
• If depression in adolescents is not properly treated, the symptoms of depression become more severe without realizing it and penetrate deeply into daily life, which can lead to failure to perform normal daily activities and ruin their entire life.
Diagnosis, signs and symptoms of depression in children and adolescents
• Have at least 5 or 5 or more of the symptoms listed in paragraphs 1 to 11 below, or
• The symptoms persist for at least 2 weeks or
• The severity of the symptoms or
• Depression can be diagnosed when the symptoms and signs prevent normal daily activities. 1.
• thinking about death or
• Have thoughts of dying or
• Sometimes you think you’re dying,
• thinking about how to die by suicide; or
• Sometimes I try to commit suicide.
• If you experience the symptoms of depression thinking about dying like this, you should consult a doctor right away or take him to the emergency room of a hospital for psychiatric treatment.
2.
• feel sad or
• feel hopeless or
• Symptoms of crying for no reason may persist.
3.
• lack of self-esteem • Feeling guilty for no reason
• I feel that I am no longer a good person.
4.
• Living has no meaning
• I don’t think anything better will happen to me in the future.
5.
• No feeling.
6.
• Losing interest in studies, social activities, physical activities, or extracurricular activities that you loved very much
• I no longer hang out with my close friends.
• Spending time alone and lonely.
7.
• Difficulty deciding when to do something
• Not starting or being unable to do anything new.
• There is a clear loss of memory and difficulty concentrating.
8.
• Your nerves become more sensitive • Get angry over trifles
• Overreact.
9.
• Sleeping too much or too little than normal
• Can eat more or less food than usual.
• Abnormal weight gain or loss.
10.
• Tired all the time for no apparent reason.
11.
• Some adolescent children with depression may have problems such as substance abuse, alcoholism, indiscretion of the opposite sex, school problems, or poor grades;
• You may have problems with your relationships with family or friends,
• Can be rebellious and destructive to authorities or parents.
If a child or adolescent is suspected of having depression
① Tell a trusted member of your family or friends that you think you are depressed, and consult with a specialist or doctor who can receive treatment for depression.
② Otherwise, receive diagnostic treatment from the pediatrician immediately.
③ Get help from school counselors, nurses, and social workers.
④ Seek help from a psychiatrist.
⑤ Seek the help of a priest, pastor, or rabbi who is qualified for counseling.
⑥ It is important to seek help and treatment from a doctor before symptoms worsen.
⑦ Weakness of mind and body, lack of sound self-esteem, problems with school studies or extracurricular activities, and not trying to do well or not doing anything at all may be symptoms of depression.
⑧ Most of the adolescent children with depression are treated well with counseling, counseling, or antidepressant medications.
⑨ Depression is a relatively common disease and can affect anyone, young or old. If you think you are depressed, you should seek professional help and treatment as soon as possible. Blood test may indicate early-onset depression in teens. The Los Angeles Times (4/18/2012), Healy reports
Treatment of Depression in Sub-Adolescents drugs used to Treat depression
• o Fluoxetine,
o Sertraline,
o Fluvoxamine,
o Citalopram,
o Escitalopram,
o There are several types such as Antitriptylin.
• Paroxetine and Imipramine have no therapeutic effect and are said to be harmful. Reference: http://www.jwatch.org/fw110644/2015/09/18/reanalysis-paroxetine-ineffective-and-harmful-treating?query=pfwTOC#sthash.baZesF4R.dpuf
• One or more antidepressant medications can be selected and used for treatment.
• However, according to a study by Irv Kirsch of University of Hull in February 2008, most drugs used to treat depression are effective in treating severe depression, but not in treating mild depression.
• Major Depressive Disorder is sometimes treated with LEXAPRO (Ecitalopram oxalate).
Figure 3-249. The rate of use of antidepressant medications is higher among adolescent girls than among adolescent boys. (The number above is the number of children treated with antidepressant medications out of 1,000 adolescent children aged 10 to 19.) Source-Medico Health Solutions Inc. and Elsevier Medical News, 2007
출처와 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
-
Neurology in Pediatrics, P. F. Bray, Yearbook Medical Publishers
-
Behavior Disorders in Children, Bakwin and Bakwin
- 소아과학 대한교과서
- 의학 용어사전 대한 의사 협회
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine